People need to be able to obtain and utilise a healthy amount and balance of nutrients. Without this, they can suffer severe impacts to their health and well-being. This building block explains malnutrition and its causes, prevalence and consequences.
Malnutrition: deficiencies, excesses or imbalances in the energy, macronutrients or micronutrients that a person obtains, either because their diet is lacking or because their body is not able to fully absorb the nutrients from the foods eaten, e.g. due to illness1,2,3.
Undernutrition: deficiencies of a particular component of food, usually due to insufficient intake and/or absorption of that component. This usually refers to energy (often measured in calories) or macronutrients (such as protein, carbohydrates, or fat), but can also refer to micronutrients (vitamins or minerals)2.
Overnutrition: excesses of energy or a particular nutrient. Overnutrition generally refers to excessive intake of energy, but it can sometimes be used to refer to excessive intake of one or more other dietary components such as specific macronutrients or micronutrients. Overnutrition in terms of energy often results in being overweight or obese2.
Macronutrients: fats, proteins and carbohydrates (starch, fibre, sugar) that are needed for a wide range of bodily functions and processes2.
Micronutrients: vitamins and minerals required by the body in smaller amounts for good health2.
Micronutrient deficiency: not getting enough of one or more micronutrients. This can happen even if a person is getting sufficient energy from their diet2.
Multiple burden of malnutrition: the simultaneous presence of more than one form of malnutrition in an individual, household or population4,5.
Non-communicable diseases: non-communicable diseases are diseases which are not passed from person to person. They are often long lasting and generally progress slowly. Examples include cardiovascular diseases, cancer, chronic respiratory diseases and diabetes6. Unhealthy diets are one of the major risk factors for non-communicable diseases7.
FAO Food Security Programme. An Introduction to the Basic Concepts of Food Security. (2008). Available at: http://www.fao.org/docrep/013/al936e/al936e00.pdf. (Accessed: 4th April 2018)
World Health Organization. Double burden of malnutrition. (2017). Available at: http://www.who.int/nutrition/double-burden-malnutrition/en/. (Accessed: 4th April 2018)
World Health Organization. Major NCDs and their risk factors. (2016). Available at: http://www.who.int/ncds/introduction/en/. (Accessed: 4th April 2018)
Malnutrition is a major driver of death and disease worldwide. Both consuming too much food and not getting enough cause problems and are exacerbated by inequalities in access to food of sufficient quality and quantity, despite the world producing enough food to feed everyone an adequate diet1. The effects of malnutrition are wide-ranging, from suboptimal health for individuals to widespread, severe deprivation and extreme suffering, such as in famines.
This building block will explore what malnutrition is and why it is a problem in all its forms, for both individuals and society.
The World Health Organisation (WHO)2 defines malnutrition as: “Deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients.”
The United Nations Children's Fund (UNICEF)3 says: “People are malnourished if their diet does not provide adequate nutrients for growth and maintenance or if they are unable to fully utilize the food they eat due to illness (undernutrition). They are also malnourished if they consume too much energy (overnutrition).”
The Food and Agriculture Organisation of the United Nations (FAO) gives the following definition4: “Malnutrition results from deficiencies, excesses or imbalances in the consumption of macro- and/or micronutrients.”
In short, malnutrition occurs when there are deficiencies, excesses or imbalances in the energy, macronutrients or micronutrients that a person obtains. This might happen because:
Their diet does not contain a sufficient variety of foods to provide nutrients in the appropriate amounts, either providing less than or more than is appropriate3.
Their body is unable to absorb or make use of certain nutrients optimally3. For example, various intestinal worms can cause loss of iron and protein and decreased absorption of nutrients5. Diarrhoea due to poor sanitation can also lead to poor absorption of nutrients6.
Their body loses too much of particular nutrients, even if the nutrients are present in the diet. For example, heavy menstrual bleeding can cause high iron loss.
A state of balanced nutrition requires suitable levels of many different nutrients in a diet, depending on individual bodily requirements. Malnutrition therefore takes many different forms, as people can consume inappropriate levels of various nutritional components. Nutrients can have maximum appropriate levels (e.g. added sugar7), minimum required levels (e.g. fibre8), or both minimum and maximum recommended limits (e.g. many vitamins and minerals9). Nutrients to which malnutrition can apply include:
Total energy, often measured in calories.
Macronutrients, which comprise:
Protein
Fat
Carbohydrate (which includes starch, fibre and sugar)
Micronutrients – both vitamins and minerals. Examples of micronutrients include:
Vitamin A
Iron
Iodine
Overnutrition means that there is too much of a component, and undernutrition means that there is not enough.
Malnutrition can cause ill health and severely affect people’s lives in many ways. This can have knock-on social and economic effects. Globally, malnutrition is estimated to cost the economy around 5% of economic output, an estimate that only accounts for lost labour productivity and direct healthcare costs10.
The effects of undernutrition are widespread and can impact whole communities. Undernutrition kills: in 2011, 45% of deaths in children under 5 years were linked to malnutrition11, a figure cited in the Global Nutrition Report 201612.
Undernutrition can increase people’s susceptibility to other forms of ill health. For example, being underweight can weaken the immune system13,14.
The cost of undernutrition and micronutrient deficiencies to the global economy, measured in terms of healthcare costs and productivity losses, could be around 2-3% of economic output10. Certain individual countries can be more strongly affected, e.g. child undernutrition is estimated to cost the Democratic Republic of Congo around 4.5% of its GDP15 and Malawi 10.3% of its GDP16.
Undernutrition in the form of hunger and macronutrient deficiencies
People who don’t obtain enough energy to enable them to maintain their body weight and carry out any necessary physical activity are at risk of ill health. The FAO calculates the threshold for undernourishment (its measure of hunger) based on the proportion of people in a country not getting enough energy to conduct “sedentary or light activities”4. The threshold varies between countries, ranging from 1,650 to more than 1,900 kilocalories per day, depending on the population’s composition by age and sex17. However, many people work in physically demanding jobs and will therefore need more energy than this if they are to avoid hunger18,17.
Energy deficiency can cause problems with growth such as wasting (a person being too thin for their height by more than two standard deviations compared to the reference population19), stunting (a child being too short for their age by more than two standard deviations compared to the reference population19) and underweight (in children, underweight means having a low weight for one’s age by more than two standard deviations compared to the reference population19; in adults, underweight means having a Body Mass Index below 18.5 – Body Mass Index is a metric that accounts for both the height and weight of the individual13).
The burden of health problems can be measured in various ways, including the numbers of people affected and the number of lost Disability-Adjusted Life Years (DALYs)20. One DALY can be thought of as one lost year of healthy life21. In 2016, around 2.3 billion years of healthy life were lost to all causes22.
Child wasting affected 51 million children under 5 years old, worldwide, in 201723 and caused 3.6% of DALYs in 201624. Child stunting affected 151 million children under 5 years old, worldwide, in 201723 and caused 0.6% of DALYs in 201624. Child underweight caused 1.4% of DALYs in 201624. Stunting is linked to the disruption of healthy brain development25.
As well as hunger arising from insufficient energy intake, deficiency in protein can lead to kwashiorkor (swelling under the skin and loss of muscle mass), marasmus (loss of fat and muscle) and sarcopenia (loss of muscle mass, particularly in older people). 12% of the global population is estimated to be currently at risk of protein deficiency26. Protein-energy malnutrition causes 0.9% of globally lost healthy years of life24.
Hunger can keep people trapped in a cycle of poverty, while poverty also drives hunger. Being less able to work because of illness and a lack of energy, hungry people are less able to earn money to buy enough food, invest in farming or maintain sanitary living conditions. Undernourishment also undermines physical and cognitive development, adding to the cycle of poverty. Chronically malnourished children often grow up to have low incomes as adults, increasing their likelihood of remaining poor and hungry27.
To read more about food security and how it relates to malnutrition, see the Foodsource building block What is food security?
Undernutrition in the form of micronutrient deficiencies
Globally, more than 2 billion people have at least one chronic micronutrient deficiency28,25. Two of the most serious micronutrient deficiencies worldwide are iron and iodine, affecting roughly 2 billion people each29,30. Vitamin A deficiency is also important: between 1995 and 2005, 33% of preschool-age children and 15% of pregnant women were estimated to be at risk, with particularly high prevalence in Africa and South-East Asia, for preschool-age children, and Western Pacific and South-East Asia, for pregnant women31.
Some examples of different forms of micronutrient deficiency are given in the table below2,32.
One paper estimates that around 3.5 billion people are at risk of calcium deficiency, due to inadequate dietary supply of calcium28. 0.14% of global DALYs are attributed to a diet low in calcium (note, however, that this may be an underestimate: in the data source, all of these DALYs are due to colon and rectum cancer; no DALYs from other known side-effects of calcium deficiency, such as rickets, appear to be included)24.
1.1 billion people are estimated to be at risk of zinc deficiency due to inadequate dietary supply of zinc28. 0.095% of global DALYs are attributed to zinc deficiency24.
33% of preschool-age children and 15% of pregnant women were estimated to be at risk of Vitamin A deficiency between 1995 and 200531. 0.17% of global DALYs are attributed to vitamin A deficiency24. Many countries have little data or outdated data33.
Unknown global prevalence due to insufficient data. Risk factors include lack of animal products in the diet and poor absorption due to aging or infection36.
If a person consumes more energy than they need, they can become overweight or obese38. As a rough guide, for adults, overweight refers to having a body mass index of 25 or more, but less than 30, and obesity refers to having a body mass index of 30 or more39,40,41.
Overweight and obesity increase the risk of many non-communicable diseases, including heart disease, stroke, some cancers, type 2 diabetes and musculoskeletal disorders such as osteoarthritis42,43,44,45,41.
A review study found that the risk of premature death (totalled across all causes) increases as a person’s body mass index increases above 25 (the risk of premature death also increases for a body mass index below 20)46. In 2015, around 4 million deaths were attributed to overweight and obesity, of which nearly 40% were in people who were overweight but not obese. Most of these 4 million deaths were due to cardiovascular disease47.
The economic effects of obesity and resultant diseases can include greater healthcare costs, loss of income, absence from work and higher disability insurance premiums48,12,45.
As well as consequences that follow directly from being overweight, prejudice in society can lead to people who are overweight suffering from negative social effects. These effects include discrimination, bullying, avoidance of healthcare services due to perceived bias, lower wages and higher social isolation49,45. In contrast, however, overweight can be regarded as a status symbol in some countries, including many sub-Saharan African countries50.
Overnutrition is also sometimes used to refer to excessive intake of a particular macronutrient or micronutrient. For example, eating a lot of sugar can increase the risk of tooth decay51, too much saturated fat can increase the risk of heart disease52 and too much selenium can cause selenosis, affecting hair and nails53.
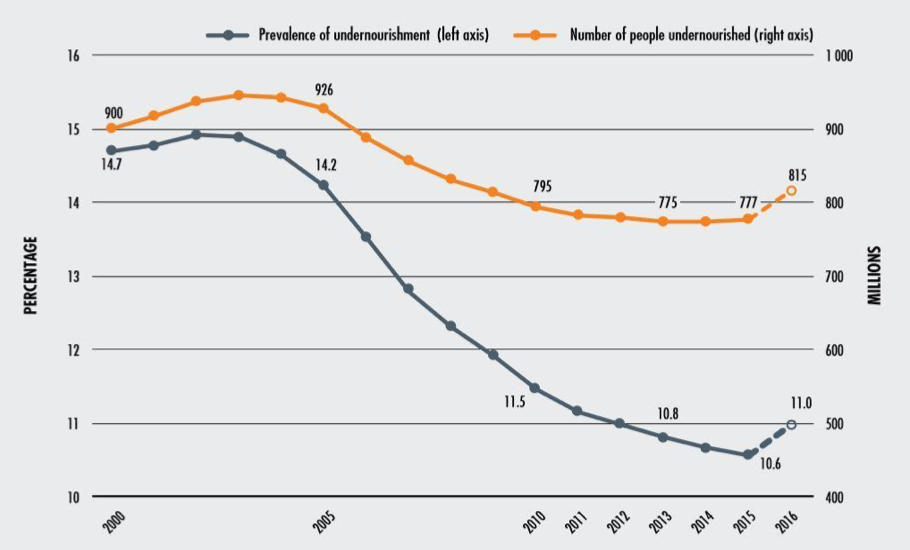
In 2016, 800 million people did not get enough energy, i.e. suffered from hunger12. While both the proportion and absolute number of undernourished (as in hungry) people have fallen since the early 2000s, the number of undernourished people may have risen slightly in recent years, as shown below. The rise has been attributed to several factors, including conflicts, droughts and economic slowdowns54.
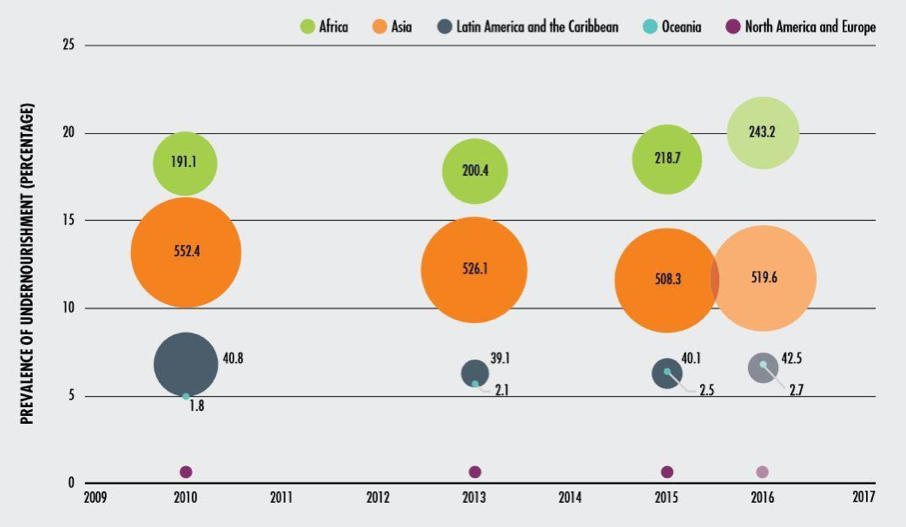
Hunger is most severe in some sub-Saharan African countries and is also moderately widespread in some parts of Asia, parts of the Middle East and some central and south American countries55. As shown below, Africa has the highest proportion of undernourished people, but Asia has the most undernourished people in absolute terms. Some people in relatively wealthy countries are also hungry. For example, 3% of the UK population was estimated to be undernourished (as in hungry) in 201556.
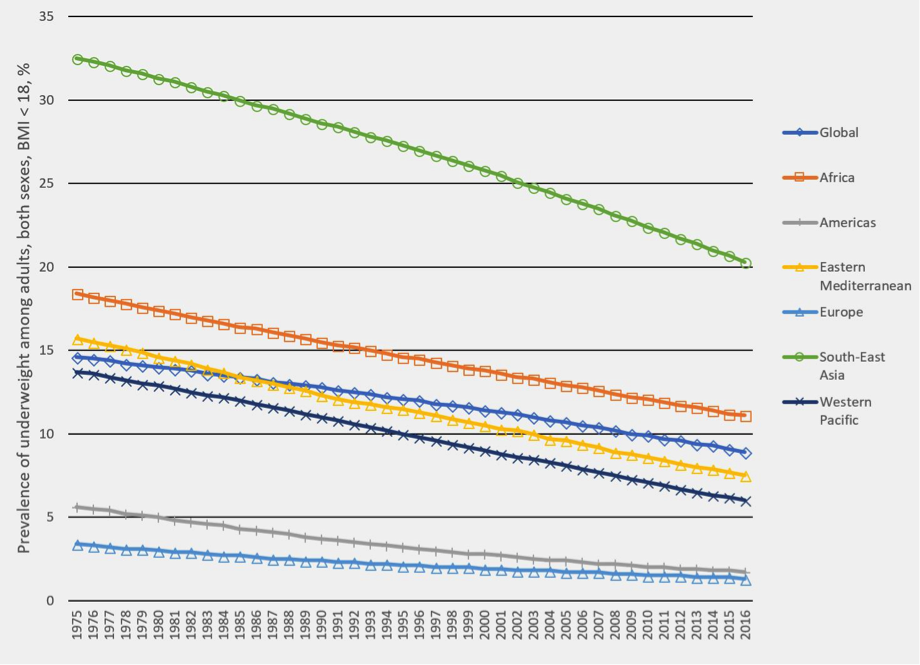
Undernourishment (as insufficient energy or macronutrient intake) can lead to underweight, i.e. low Body Mass Index. The proportion of adults with a Body Mass Index less than 18 is currently highest in South-East Asia and has been falling across all regions since 1975, as shown below.
Image
Prevalence of underweight among adults 18+ years of age, measured by BMI < 18, by WHO region, both sexes, 1975 to 2016. Prevalence is defined as % of the relevant population. This is the crude estimate (as opposed to the age-standardised estimate). Data source57: World Health Organization. 2017. Global Health Observatory data repository - Prevalence of underweight among adults, BMI < 18, crude - Estimates by WHO region. Graph prepared by the Food Climate Research Network.
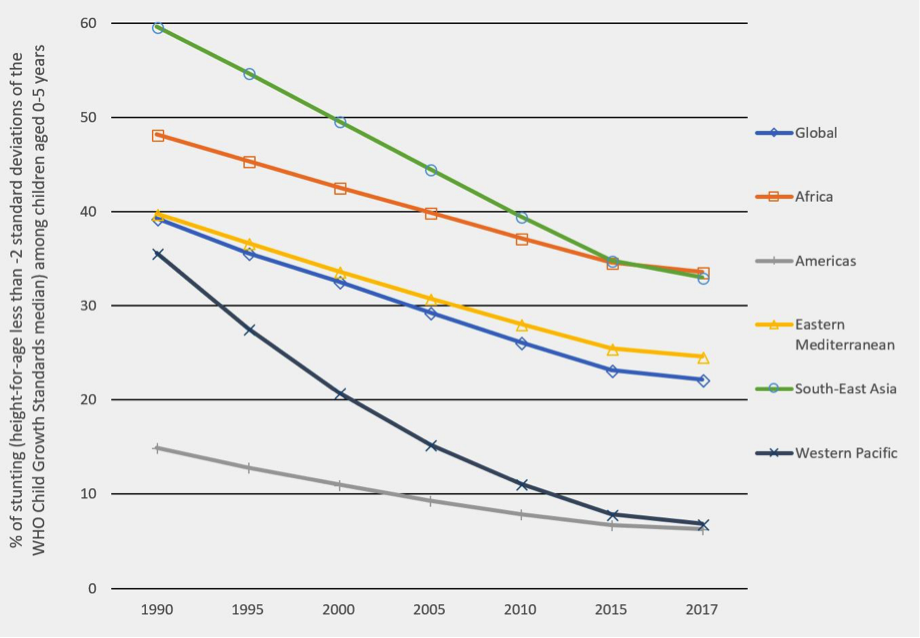
Chronic malnutrition leading to stunting (low height for age) has particularly serious consequences for future health when it happens in young children58. The prevalence of stunting in children aged 0 to 5 years has been falling across all regions since 1990. Child stunting is currently most prevalent in Africa and South-East Asia, as shown below.
Image
Prevalence of child stunting (height-for-age less than -2 standard deviations of the WHO Child Growth Standards median) as a percentage of children aged 0-5 years, 1990 to 2017. The data source does not include Europe. Data source59: World Health Organization. 2018. Global Health Observatory data repository - Global and regional trends by WHO Regions, 1990-2025 - Stunting: 1990-2025. Graph prepared by the Food Climate Research Network.
Around 2 billion people suffer from micronutrient deficiencies25. In 2006, WHO found that micronutrient deficiencies were widespread in industrialised countries, but even more common in developing countries. Young children and women of reproductive age are at high risk compared to other demographic groups. Anaemia was found to be particularly prevalent in South-East Asia (at 57% of the population), Africa (46%) and the Eastern Mediterranean (45%), and lowest in Europe (10%). Insufficient iodine intake was particularly prevalent in Europe (57%) and the Eastern Mediterranean (54%), and lowest in the Americas (10%)36.
In 2016, more than 1.9 billion adults (39% of adults) were overweight. Of these, over 650 million (13% of adults) were obese45. Furthermore, 41 million children under 5 and 340 million people aged between 5 and 19 were overweight or obese41.
The percentage of overweight adults varies highly between countries, ranging from, for example, 18% in Vietnam to 89% in Nauru (these figures are age-standardised estimates for 2016). Countries with a high percentage of overweight people can be found across the world, including Saudi Arabia (70%), the United States of America (68%), Mexico (65%), Australia (65%), the United Kingdom (64%) and Argentina (63%)60.
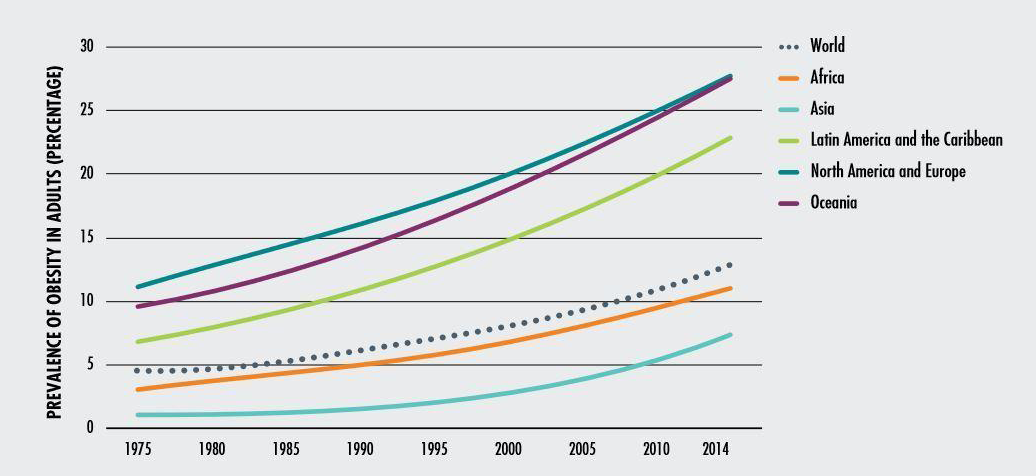
Adult obesity is rising on all continents, as shown below.
In low- and middle-income countries, obesity is generally highest in urban areas61. In low income countries, people with a higher socioeconomic status are more likely to be obese than people with a lower socioeconomic status. This is true of both men and women. In middle income countries, obesity has a mixed correlation with socioeconomic status for men while obesity and socioeconomic status are negatively correlated for women62.
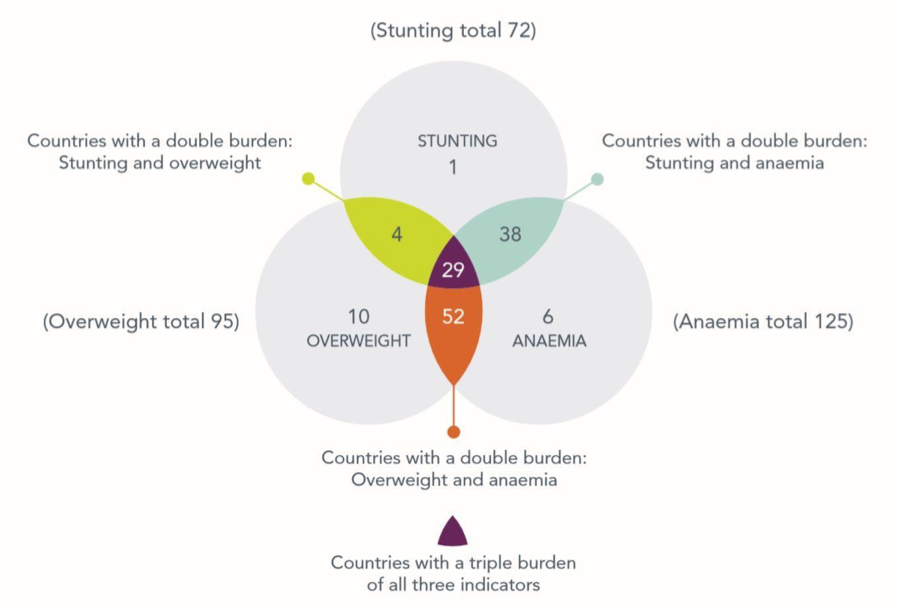
The “multiple burden” of malnutrition refers to more than one form of malnutrition present in the same individual, household or population63,54. 88% of countries for which there are data are simultaneously experiencing serious burdens of either two or three of the following forms of malnutrition: childhood stunting, anaemia in women of reproductive age and overweight in adult women25. The figure below illustrates this.
Image
Number of countries facing burdens of malnutrition. Image source25: Development Initiatives. Global Nutrition Report 2017: Nourishing the SDGs. (2017). The International Food Policy Research authorises the use of this material subject to the terms and conditions on its website.
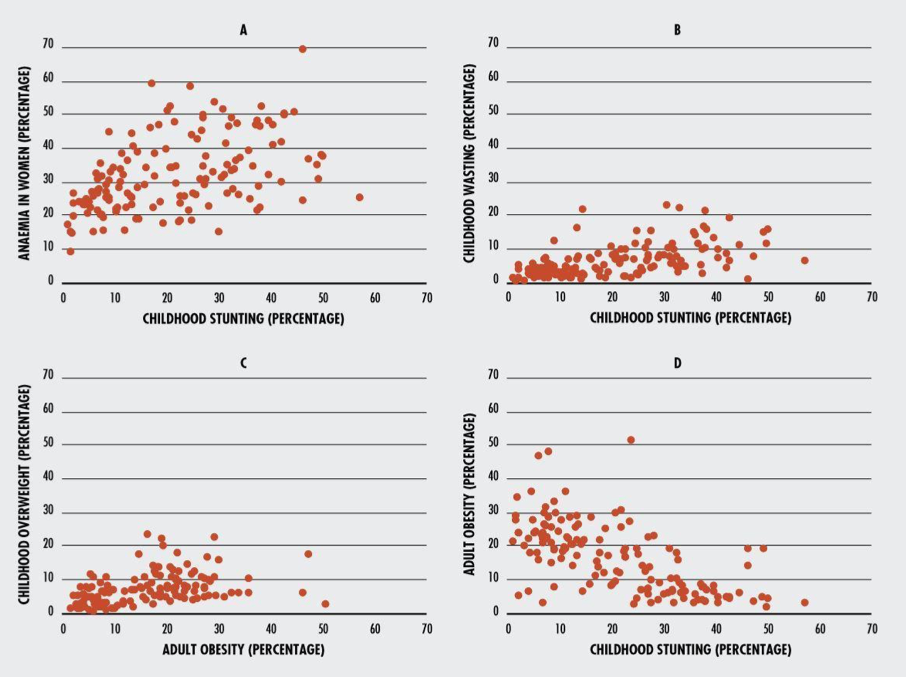
Section D of the figure below shows that, while adult obesity and childhood stunting are inversely correlated, they are often present in the same country.
It is also possible for an individual to simultaneously have more than one form of malnutrition3. For example, they could be overweight because of excess energy intake, but deficient in iron because of insufficient intake or absorption of iron64.
World Hunger Education Service. World Hunger, Poverty Facts, Statistics 2016 - World Hunger News. (2016). Available at: https://www.worldhunger.org/2015-world-hunger-and-poverty-facts-and-statistics/. (Accessed: 4th April 2018)
FAO Food Security Programme. An Introduction to the Basic Concepts of Food Security. (2008). Available at: http://www.fao.org/docrep/013/al936e/al936e00.pdf. (Accessed: 4th April 2018)
World Health Organization. Soil-transmitted helminth infections. (2017). Available at: http://www. who.int/mediacentre/factsheets/fs366/en/. (Accessed: 4th April 2018)
WHO technical staff. Water, sanitation and hygiene interventions and the prevention of diarrhoea. WHO e-Library of Evidence for Nutrition Actions (2011). Available at: http://www.who.int/elena/titles/bbc/wsh_diarrhoea/en/. (Accessed: 7th June 2018)
British Nutrition Foundation. Dietary fibre. (2018). Available at: https://www.nutrition.org.uk/healthyliving/basics/fibre.html. (Accessed: 7th June 2018)
International Food Policy Research Institute. Global Nutrition Report 2016: From Promise to Impact: Ending Malnutrition by 2030. (2016). doi:10.2499/9780896295841
Rytter, M. J. H., Kolte, L., Briend, A., Friis, H. & Christensen, V. B. The immune system in children with malnutrition - A systematic review. PLoS ONE (2014). doi:10.1371/journal.pone.0105017
Relief Web. New Study Reveals Economic Toll Of Malnutrition In Democratic Republic Of Congo - Democratic Republic of the Congo. (2017). Available at: https://reliefweb.int/report/democratic-republic-congo/new-study-reveals-economic-toll-malnutrition-democratic-republic. (Accessed: 4th April 2018)
United Nations World Food Programme. New Study Reveals Huge Impact Of Hunger On Economy Of Malawi. (2015). Available at: https://www.wfp.org/news/news-release/new-study-reveals-huge-impact-hunger-economy-malawi-0. (Accessed: 4th April 2018)
Hickel, J. The hunger numbers: are we counting right? The Guardian (2015). Available at: https://www.theguardian.com/global-development-professionals-network/2015/jul/17/the-hunger-numbers-are-we-counting-right. (Accessed: 4th April 2018)
World Health Organization. Disability-adjusted life years (DALYs). (2017). Available at: http://www.who.int/gho/mortality_burden_disease/daly_rates/text/en/. (Accessed: 4th April 2018)
World Health Organization. Metrics: Disability-Adjusted Life Year (DALY). (2014). Available at: http://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/. (Accessed: 4th April 2018)
Roser, M. & Ritchie, H. Burden of Disease - Our World in Data. (2016). Available at: https://ourworldindata.org/burden-of-disease. (Accessed: 4th April 2018)
Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization. University of Washington (2016). Available at: https://vizhub.healthdata.org/gbd-compare/. (Accessed: 4th April 2018)
Medek, D. E., Schwartz, J. & Myers, S. S. Estimated Effects of Future Atmospheric CO2 Concentrations on Protein Intake and the Risk of Protein Deficiency by Country and Region. Environ. Health Perspect.125, (2017).
de Benoist, B., Andersson, M., Egli, I., Takkouche, B. & Allen, H. Iodine status worldwide. WHO Glob. Database Iodine Defic. Geneca World Heal. Organ. 1–12 (2004).
World Health Organization. Global prevalence of vitamin A deficiency in population at risk: 1995-2005. (2013). Available at: http://www.who.int/vmnis/database/vitamina/x/en/. (Accessed: 4th April 2018)
Pecukonis, O. Global data on vitamin A status is critical for program decisions but often outdated, reveals new study - Nutrition International. Nutrition International (2017). Available at: https://www.nutritionintl.org/2017/06/global-data-vitamin-status-critical-program-decisions-often-outdated-reveals-new-study/. (Accessed: 4th April 2018)
Rabinowitz, S. S. Pediatric Beriberi: Background, Pathophysiology, Epidemiology. Medscape (2014). Available at: https://emedicine.medscape.com/article/984721-overview. (Accessed: 4th April 2018)
Foster, M. R. & Kolaski, K. Spina Bifida: Background, Pathophysiology, Etiology. Medscape (2016). Available at: https://emedicine.medscape.com/article/311113-overview#a5. (Accessed: 4th April 2018)
Centers for Disease Control and Prevention. Defining Adult Overweight and Obesity. (2016). Available at: https://www.cdc.gov/obesity/adult/defining.html. (Accessed: 7th June 2018)
World Health Organization. Obesity and overweight. (2017). Available at: http://www.who.int/mediacentre/factsheets/fs311/en/. (Accessed: 4th April 2018)
Cancer Research UK. Our policy on obesity and diet. (2017). Available at: http://www.cancerresearchuk.org/about-us/we-develop-policy/our-policy-on-preventing-cancer/our-policy-on-obesity-and-diet. (Accessed: 4th April 2018)
Centers for Disease Control and Prevention. The Health Effects of Overweight and Obesity. (2015). Available at: https://www.cdc.gov/healthyweight/effects/index.html. (Accessed: 4th April 2018)
Harvard T.H. Chan School of Public Health. Obesity Consequences. Harvard T.H. Chan School of Public Health, Available at: https://www.hsph.harvard.edu/obesity-prevention-source/obesity-consequences/. (Accessed: 4th April 2018)
The Global BMI Mortality Collaboration et al. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet388, 776–786 (2016).
Global Burden of Disease 2015 Obesity Collaborators et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. (2017). doi:10.1056/NEJMoa1614362
The Obesity Society. Obesity, Bias, and Stigmatization. Available at: http://www.obesity.org/obesity/resources/facts-about-obesity/bias-stigmatization. (Accessed: 4th April 2018)
Scott, A., Ejikeme, C. S., Clottey, E. N. & Thomas, J. G. Obesity in sub-Saharan Africa: Development of an ecological theoretical framework. Health Promot. Int. (2013). doi:10.1093/heapro/das038
National Institutes of Health. Selenium — Health Professional Fact Sheet. (2018). Available at: https://ods.od.nih.gov/factsheets/Selenium-HealthProfessional/. (Accessed: 4th April 2018)
World Food Programme. Hunger Map 2015. (2015). Available at: http://documents.wfp.org/stellent/groups/public/documents/communications/wfp275057.pdf?_ga=2.7179323.82857225.1519983745-547711402.1519983745. (Accessed: 4th April 2018)
The World Bank. Prevalence of undernourishment (% of population). World Bank Open Data Available at: https://data.worldbank.org/indicator/sn.itk.defc.zs. (Accessed: 7th June 2018)
World Health Organization. Global Health Observatory data repository - Prevalence of underweight among adults, BMI < 18, crude - Estimates by WHO region. (2017). Available at: http://apps.who.int/gho/data/view.main.NCDBMILT18CREGv?lang=en. (Accessed: 12th June 2018)
World Health Organization. Stunting in a nutshell. WHO (2015). Available at: http://www.who.int/nutrition/healthygrowthproj_stunted_videos/en/. (Accessed: 12th June 2018)
World Health Organization. Global Health Observatory data repository - Global and regional trends by WHO Regions, 1990-2025 - Stunting: 1990-2025. (2018). Available at: http://apps.who.int/gho/data/view.main.NUTWHOSTUNTINGv?lang=en. (Accessed: 12th June 2018)
World Health Organization. Global Health Observatory (GHO) data repository - Overweight and obesity. (2017). Available at: http://www.who.int/gho/ncd/risk_factors/overweight/en/. (Accessed: 4th April 2018)
Ford, N. D., Patel, S. A. & Narayan, K. M. V. Obesity in Low- and Middle-Income Countries: Burden, Drivers, and Emerging Challenges. Annu. Rev. Public Health38, 145–164 (2017).
Dinsa, G. D., Goryakin, Y., Fumagalli, E. & Suhrcke, M. Obesity and socioeconomic status in developing countries: A systematic review. Obes. Rev. (2012). doi:10.1111/j.1467-789X.2012.01017.x
World Health Organization. Double burden of malnutrition. (2017). Available at: http://www.who.int/nutrition/double-burden-malnutrition/en/. (Accessed: 4th April 2018)
Data visualisation from Global Burden of Disease: GBD Compare
Book: Hidden Hunger, by Hans Konrad Biesalski (2013)
Acknowledgements
Suggested citation
Breewood, H. (2018). What is malnutrition? (Foodsource: building blocks). Food Climate Research Network, University of Oxford.
Written by
Helen Breewood, Research Assistant at the Food Climate Research Network, University of Oxford
Edited by
Sam Lee-Gammage, Research and Communications Officer at the Food Climate Research Network, University of Oxford
Tara Garnett, Director of the Food Climate Research Network, University of Oxford
Reviewed by
Shauna Downs, Assistant Professor, Rutgers School of Public Health
Jennie Macdiarmid, Professor in Sustainable Nutrition and Health, University of Aberdeen
Suneetha Kadiyala, Associate Professor in Nutrition-Sensitive Development at the London School of Hygiene & Tropical Medicine
With additional thanks to
Walter C. Willett, Professor of Epidemiology and Nutrition at the Harvard T.H. Chan School of Public Health, and Jessica Fanzo, Bloomberg Distinguished Associate Professor of Global Food & Agricultural Policy and Ethics at the Johns Hopkins Berman Institute of Bioethics, for advice on definitions and pointing us towards relevant resources
Reviewing and advising do not constitute an endorsement. Final editorial decisions, including any remaining inaccuracies and errors, are the sole responsibility of the Food Climate Research Network.





Comments (0)